
Lateral Elbow Pain and Lateral Epicondylalgia
Lateral epicondylalgia, also known as tennis elbow, is an overuse injury involving the common origin tendon of the wrist and finger extensors. Patients with this condition often report pain in the lateral elbow exacerbated by gripping, lifting, or manipu- lating objects with their hands.
Previously thought to be a condition of inflammation (lateral epicondylitis), new research shows a lack of inflammatory cells in this condition. Instead, lateral epicondylalgia is considered a degenerative condition and one of dysfunctional, immature healing of the tendon(5,6). Tendons have been shown to remodel and heal along the lines of stress from exercise and appropriate loading(7).
4-7 cases per 1000 patients experience the condition and lateral epicondylalgia has a 1-3% incidence within the general population(1,2).
The condition primarily effects the dominant arm of individuals between 35-54 years old1. Amateur tennis players, patients with poor posture, frequent computer use, and manual tasks involv- ing force and repetition are at greater risk for the condition(2).
The majority of patients reports resolution of their symptoms by 1 year but may range up to 24 months(1).
Physical Therapy interventions have been shown to accelerate this recovery process and have been shown to be more cost effective than a wait and see approach or a corticosteroid injection(9).
Elbow Pain and Physical Therapy Treatments

Review articles do not support the use of Physical Therapy modalities including ultrasound and iontophoresis in the treatment of lateral epicondylalgia(4).
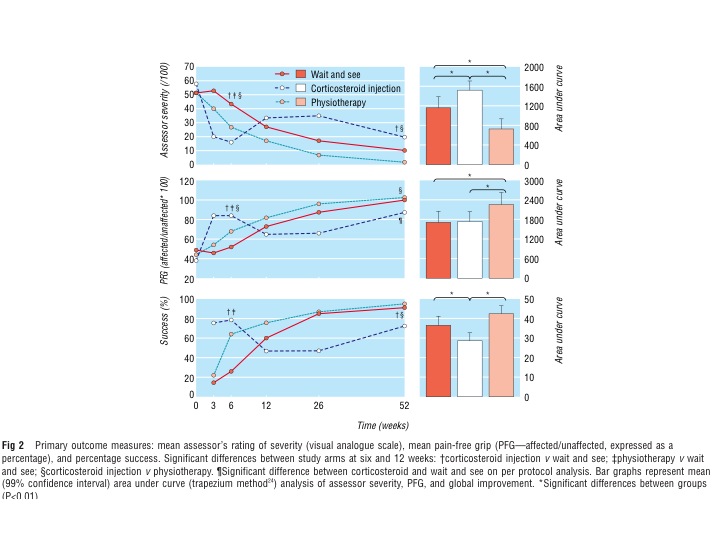
Corticosteroid injections have been advocated for short term relief by many studies. While experiencing early relief, patients undergoing corticosteroid injections have a higher recurrence rate (72%) compared to a wait and see (10%) or Physical Therapy treatments (4%). (3)
Recent systematic report strong evidence against the utilization of platelet rich plasma (PRP) injections in patients with lateral elbow tendinopathy(12).
Evidence reviews on the topic of lateral elbow pain advocate for a multimodal Physical Therapy treatment model including spinal and extremity joint manipulation/ mobilization, soft tissue treatments, and strengthening exercises(4,13).

Physical Therapy Evidence
A manual physical therapy approach combined with exercise has been shown to accelerate a patient’s recovery by reducing pain and disability in the short term. Medical evidence has also shown patients receiving this treatment approach have the lowest recur- rence rate of pain and medication use(10,11).
Conversely, poorer long term outcomes and higher recurrence rates have been documented in patients receiving corticosteroid injections(10).
Bisset et al. reported the utilization of manual therapy and exercise is superior to wait and see and corticosteroid injection at short-term follow up11. It appears PT helps accelerate recovery and is superior to a wait and see approach.
Evidence suggests treatment of the upper quarter including the cervical, thoracic, elbow, and wrist regions may provide positive effects on patient’s pain and function(14).
When to Seek Physical Therapy Care
Patient’s with lateral elbow pain exacerbated by gripping or manipulation of the hand and wrist should be treated with a multimodal Physical Therapy treatment plan to reduce pain and disability.
References
1. Smidt N, Lewis M, Van Der Windt DA, et al. Lateral epicondylitis in general practice: course and prognostic indicators of outcome. J Rheumatol 2006;33:2053–9.
2. Shiri R, Viikari-Juntura E, Varonen H, et al. Prevalence and determinants of lateral and medial epicondylitis: a population study. Am J Epidemiol 2006;164:1065–74.
3. Bisset L, Beller E, Jull G, et al. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. BMJ 2006;333:939.
4. Coombes, B. et al. A new integrative model of lateral epicondylalgia. Br J Sports Med 2009;43:252–258
5. Fredberg U, Stengaard-Pedersen K. Chronic tendinopathy tissue pathology, pain mechanisms, and etiology with a special focus on inflammation. Scand J Med Sci Sports 2008;18:3–15.
6. Alfredson H, Ljung BO, Thorsen K, et al. In vivo investiga- tion of ECRB tendons with microdialysis technique–no signs of inflammation but high amounts of glutamate in tennis elbow. Acta Orthop Scand 2000;71:475–9.
7. Riley G. Chronic tendon pathology: molecular basis and therapeutic implications. Expert Rev Mol Med 2005;7:1- 25.
8. Smidt N, Assendelft WJ, van der Windt DA, et al. Corticosteroid injections for lateral epicondylitis: a systematic review. Pain 2002;96:23–40.
9. Coombes, B. et al. Economic evaluation favours physiotherapy but not corticosteroid injection as a first-line intervention for chronic lateral epicondylalgia: evidence from a randomised clinical trial. Br J Sp Med. 2015.
10. Coombes, B. Effect of Corticosteroid Injection, Physiotherapy, or Both on Clinical Outcomes in Patients With Unilateral Lateral Epicondylalgia A Randomized Controlled Trial. JAMA. 2013. 309(5):461-469.
11. Bisset L, Beller E, Jull G, Brooks P, Darnell R, Vicenzino B. Mobilisation with movement and exercise, corti- costeroid injection, or wait and see for tennis elbow: randomised trial. BMJ. 2006;333(7575):939.
12. De Vos, R. et al. Strong evidence against PRP injections for chronic lateral elbow tendinopathy. A systematic review. Br J Sp Med. 2014.
13. Fernandez-Carnero, J. et al. EXAMINATION OF MOTOR AND HYPOALGESIC EFFECTS OF CERVICAL VS THORACIC SPINE MANIPULATION IN PATIENTS WITH LATERAL EPICONDYLALGIA: A CLINICAL TRIAL. J Manipulative Ther Phys. 2011. 34(7):432-440.
14. Vicenzino, B. et al. Joint manipulation in the management of lateral epicondylalgia. A clinical commentary. JMMT. 2007. 15(1):50-56.