
Athletic Injuries
More than 10,000 athletes seek treatment for sports, recre- ation, and exercise based injuries on a daily basis(12).
7 million Americans received medical attention for sports and athletic injuries between 1997-1999(1).
Incidence of athletic injuries has been reported as 15.4-25.9 injuries per 1000 in the population(2,3).
50-80% of these injuries have been described as overuse in nature and may be prevented through the utilization of pre-participation screens(13).
Functional Movement Screen
FMS is a ranking and grading system that documents move- ment patterns that are key to normal function3. It requires individuals to move through all 3 planes of motion allowing the examiner to document both the quantity and quality of the movement pattern.
Risk factors associated with injury in athletic events including muscle imbalances, balance and proprioception impairments, and pain are assessed with each movement.
The screen allows Physical Therapists to objectively score and grade individuals for injury risk prior to participation as well as follow and reassess these at risk individuals after Physical Therapy treatment is initiated.
FMS Evidence
Plisky et al. identified an anterior side to side reach difference of greater than 4 cm on the star excursion test placed a high school basketball athlete at a 2.5 times greater risk of lower extremity injury in their season. Further, in females a compos- ite reach <94% of their limb length placed them at a 6.5 times greater risk(11).
Kiesel et al. reported a score of <14/21 was able to predict serious injury in a group of professional football players. (Specificity .91, Sensitivity .54 (+) LR 5.92 (-) LR .51)(4).
These individuals were almost 12 times (odds ratio 11.67) more likely to sustain a serious injury versus an athlete scoring higher on this testing(4).
Chorba et al. found similar findings among a group of female Division II athletes where a score of <14/21 placed the individual at a 4 times greater risk of lower extremity injury(5).
Authors have reported a 7 week (4-6/week) supervised off season conditioning program was able to improve professional football players FMS scores in previously at risk athletes. A low score on the deep squat was most predictive of a lack of success with this program(6).
Peate et al. has also reported on the impact of the FMS screen and an 8 week intervention program on a group of 433 inter- national firefighters. This program reduced the time off work due to injury by >60%(8).
Lower sensitivity values (.08), but higher specificity (.95) were found among recreational runners training for a half mara- thon scoring < or > 14/2110. These higher specificity scores may be explained by a low number of individuals scoring <14.
Letafatkar et al. indicated an almost 5 times greater risk of injury among recreationally active college students scoring <17/21(7).
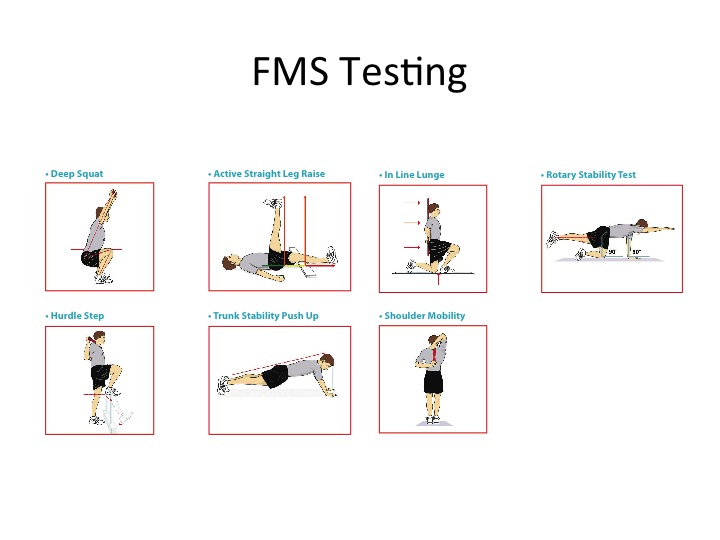
Testing
The 7 tests utilize a variety of basic positions and movements, which are though to provide the foundation for more complex athletic movements to be performed efficiently(4).
Individuals are graded and assigned a level of injury risk based on these 7 movements with a total possible score of (21).
Teyhen et al. has described moderate to good inter and intra rater reliability and acceptable levels of measurement error with the FMS(9).
References
1. Conn JM, Annest JL, Gilchrist J. Sports and recreation related injury episodes in the US population, 1997–99. Inj Prev. 2003;9(2):117-123.
2. Gotsch K, Annest JL, Holmgren P, Gilchrist J. Nonfatal sports- and recreation- related injuries treated in emergency departments—United States, July 2000–June 2001. MMWR Morb Mortal Wkly Rep. 2002;51(33):736-740.
3. Functional Movement Systems. Functionalmovement.com
4. Kiesel, K. et al. CAN SERIOUS INJURY IN PROFESSIONAL FOOTBALL BE PREDICTED BY A PRESEASON FUNCTIONAL MOVEMENT screen? N Am J Sports Phys Ther. 2007. 2(3):147-158
5. Chorba RS, Chorba DJ, Bouillon LE, Overmyer CA, Landis JA. Use of a Functional Movement Screening Tool to Determine Injury Risk in Female Collegiate Athletes. N Am J Sports Phys Ther. 2010; 5(2):47-54.
6. Kiesel K, Plisky P, Butler R. Functional movement test scores improve following a standardized off- season intervention program in professional football players. Scand J Med Sci Sports. 2011; 21(2):287-92.
7. Letafatkar, A. et al. Relationship between functional movement screening score and history of injury. International J Sp Phys Ther. 2014. 9(1):21-27.
8. Peate WF, Bates G, Lunda K, Francis S, Bellamy K. Core strength: a new model for injury prediction and prevention. J Occup Med Toxicol. 2007; 2: 3.
9. Teyhen DS, Shaffer SW, Lorenson CL, Halfpap JP, Donofry DF, Walker MJ. The functional movement screen: A Reliability Study. J Orthop Sports Phys Ther. 2012; 42(6): 530-540.
10. Hoover D, Killian CB, Bourcier B, Shannon L, Jenny T, Willis R. Predictive validity of the Functional Movement Screening in a population of recreational runners training for a half marathon. Med Sci Sports Exerc. 2008; 40(5): 219.
11. Plisky et al. Star Excursion Balance Test as a Predictor of Lower Extremity Injury in High School Basketball Players. JOSPT. 2006. 36(12):911-919.
12. National Center for Injury Prevention and Con- trol, Centers for Disease Control and Prevention. CDC Injury Research Agenda. Atlanta, GA: US Department of Health and Human Services; 2002.
13. Almeida SA, Williams KM, Shaffer RA, Brodine SK. Epidemiological patterns of musculoskeletal injuries and physical training. Med Sci Sports Exerc. 1999;31:1176-1182.