

Hip Osteoarthritis Background
Hip Osteoarthritis (OA) is considered one of the most serious musculoskeletal problems secondary to its impact on patients’ pain and disability, as well as, the economic impact on our healthcare system.
20% of the aging population will experience hip OA and the condition is a predictor of current and future func- tional disability and mortality(1,2).
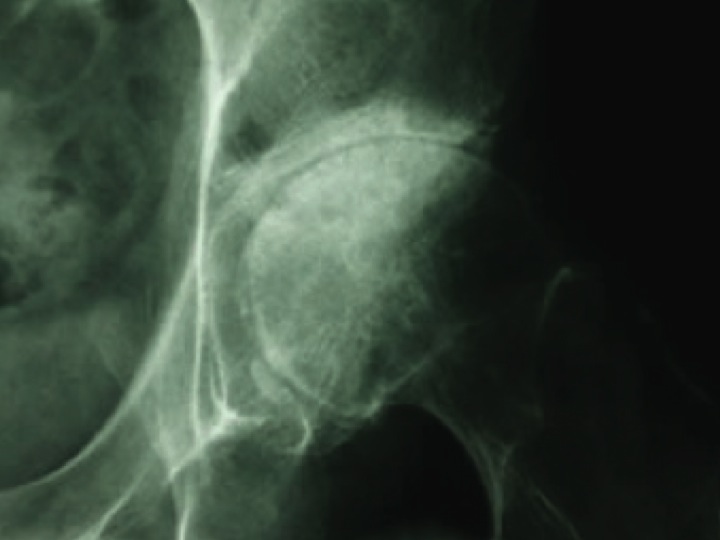
Only 20% of patients with hip OA on x ray testing will end up having a total hip replacement 11-28 years after diag- nosis. Quality conservative care is crucial for this population(3).
Physical Therapy Interventions
Clinical practice guidelines recommend the use of educa- tion, weight reduction, gait and balance training, exercise size, and manual therapy in the management of patients with hip OA(4).
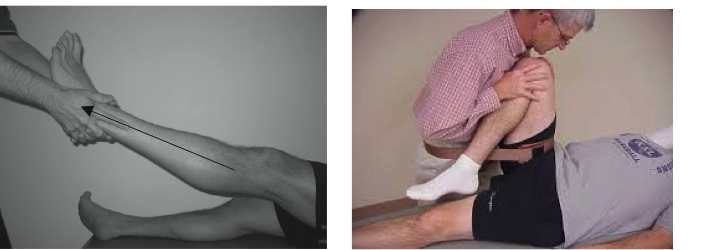
Manual therapy interventions including joint mobilizations/ manipulation reduce pain, improve ROM and reduce disability in patients who do not have severe, end stage hip OA(4).
Physical Therapy Evidence for Hip Osteoarthritis
81% of patients reported reduced pain, disability, and a high level of perceived recovery following a treatment plan of manual therapy compared to exercise alone(5).
Pinto et al. reported manual therapy and exercise were more clinically and cost effective than usual care in an evaluation of treatments for patients with hip OA(8).
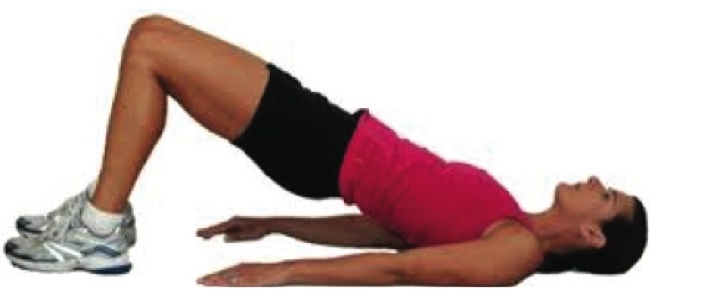
Exercise interventions including flexibility/range of motion exercise, strengthening, and aerobic exercise are supported for their impact on reduc- ing pain and disability for patients suffering from hip OA(4).
When to seek Physical Therapy care
Clinical clusters of Hip OA include one of the following(6)
All 3 findings
Pain in hip
<115 degrees hip flexion
<15 degrees hip internal rotation
All 3 findings
Pain with hip internal rotation
<60 minutes of morning stiffness
>50 years of age
Sutlive et al. reported a cluster of findings including the following demonstrated a (+)LR of 24.3 or 5.2 for 4/5 or 3/5 findings respectively(7).
Squatting as aggravating factor
(+) active hip flexion causing lateral hip pain
(+) scour test causing lateral hip or groin pain
Active hip extension causes hip pain
Passive internal rotation range of motion <25 degrees
References
1. Odding, E. et al. Determinants of locomotor disability in people aged 55 years and over: the Rotterdam Study. Eur J Epidemiol. 2001. 17(11):1033-1041
2. Nuesch, E et al. All cause and disease specific mortality in patients with knee and hip osteoarthritis: population based cohort study. BMJ. 2011.
3. Franklin, J. et al. Natural history of hip OA: A retrospective cohort study with 11-28 years of follow up. Arthritis Care Res. 2011. 63(5):689-95
4. Cibulka, M. et al. Hip Pain and Mobility Deficits – Hip Osteoarthritis. Clinical practice guidelines. JOSPT. 2009. 39(4):A1-A25.
5. Hoeksma H et al. Comparison of manual therapy and exercise therapy in osteoarthritis of the hip: a RCT. Arthrtis Rheum. 2004. 51:722-729.
6. Altman R, Alarcon G, Appelrouth D, et al. The American College of Rheumatol- ogy criteria for the classification and reporting of osteoarthritis of the hip. Arthritis Rheum. 1991;34:505-514.
7. Sutlive, T. et al. Development of a clinical prediction rule for the diagnosis of hip OA in individuals with unilateral hip pain. J Orthop Sports Phys Ther 2008;38(9):542-550.
8. Pinto, D. et al. Manual therapy, exercise therapy, or both, in addition to usual care, for osteoarthritis of the hip or knee. Economic evaluation alongside a RCT. Osteoarthritis and cartilage. 2013.