
Shoulder Pain and Impingement Background
Shoulder pain is a common source of peripheral joint pain occurring at a prevalence rate of up to 47% across all age groups and is second most common cause of musculoskeletal pain(7,9).
Symptoms of shoulder pain account for 33.2% of physician visits in the U.S. and are most frequently associated with SAIS(13). Only 50% of new shoulder problems show resolution of patient symptoms at 6 months(12)
Physical Therapy Interventions
Evidence in the medical literature supports the utilization of manual therapy to the spine and shoulder girdle in the management of shoulder pain disorders(1, 2, 3, 5, 6, 8, 10, 11).
Patients with SAIS who received thoracic spine thrust manipulations demonstrated significant decreases in pain and disability scores at 48 hours(3).
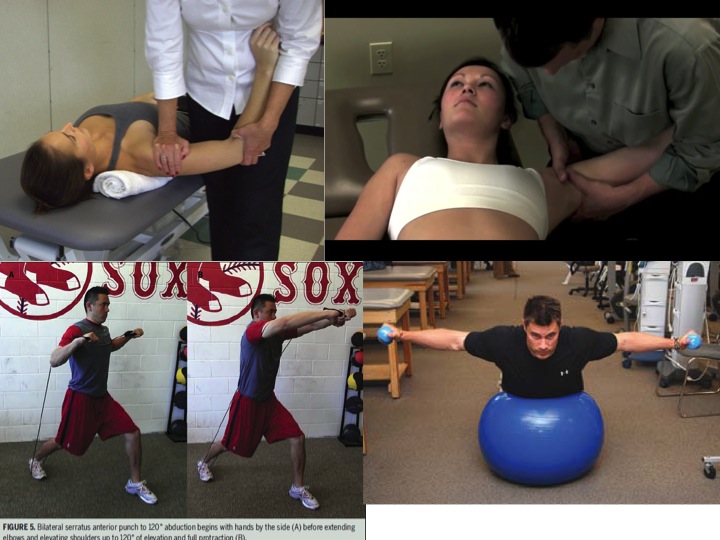
A combined program of manual therapy and upper quarter strengthening has demonstrated improved symptoms and disability in patients with SAIS(9).
Systematic reviews support the utilization of rotator cuff and scapular strengthening, in combination with manual therapy, for patients with SAIS(6,8).
Physical Therapy Evidence for Shoulder Pain Treatments
Multiple articles in the research literature describe the effectiveness of a multimodal approach to treating shoulder pain utilizing manual therapy to the upper quarter and therapeutic exercise(1, 2, 5, 6, 8, 10).
Bang et al. reported significantly greater improvements in motion, strength, pain and function in a group treated with manual therapy and exercise compared with exercise alone(1).
Manipulative physical therapy when combined with supervised exercise has been shown to produce faster improvements in pain, ROM and function in patients with SAIS compared to patients who just performed exercise or received self care alone(1, 5, 10).
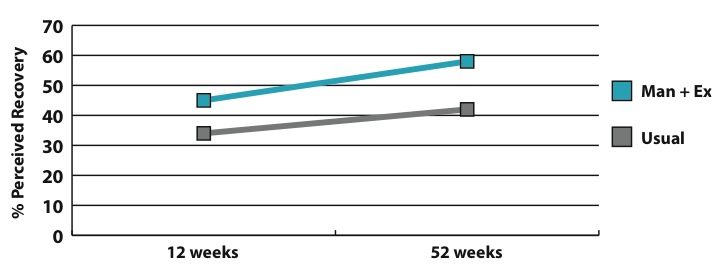
The addition of manual therapy to patients receiving usual care for their shoulder complaints accelerated their recovery to previous functional levels(2).
Specifically, the usual care group took 52 weeks to demonstrate the functional improvement noted in the manual therapy group at 12 weeks (see graph)(2).
Brox et al. has demonstrated a physical therapy program was as effective as surgical sub-acromial decompression in the treatment of stage II primary impingement(4).
When to seek Physical Therapy Care
Physicians should consider referral of patients with symptoms of shoulder pain and dysfunction associated with reaching, lifting, repetitive upper extremity activities, or over head activities.
Research supports the utilization of manual therapy and exercise in this patient population for reduction of pain and disability associated with shoulder pain. Physical Therapy combined with primary care management can accelerate recovery associated with these symptoms(1,2,5).
References
1. Bang, M. et al. Comparison of supervised exercise with and without manual physical therapy for patients with subacromial impingement syndrome. JOSPT. 2000. 30(3):126-137.
2. Bergman, G. et al. Manipulative therapy in addition to usual medical care for patients with shoulder dysfunction and pain. A RCT. Ann Int Med. 2004. 141:432-439.
3 Boyles R, et al. The short-term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. Man Ther. 2009. 14:375-380
4. Brox, J. et al. Arthroscopic surgery compared with supervised exercise in patients with rotator cuff disease (stage II impingement syndrome). BMJ. 1993. 307(6909):899-903.
5. Kachingwe A, Phillip B, Sletten E, Plunkett S. Comparison of manual therapy techniques with therapeutic exercise in the treatment of shoulder impingement: a randomized controlled pilot clinical trial. J Man Manip Ther. 2008. 16:238-247.
6. Kuhn JE. Exercise in the treatment of rotator cuff impingement: a systematic review and a synthesized evidence-based rehabilitation protocol. J Shoulder Elbow Surg. 2009. 18:138-160
7. Luime J. et al. Prevalence and incidence of shoulder pain in the general population; a systematic review. Scand J Rheumatol. 2004. 33:73–81.
8. Michener, L. et al. Effectiveness of Rehabilitation for Patients with Subacromial Impingement Syndrome: A Systematic Review. J Hand Ther. 2004. 17:152–164.
9. Picavet H. et al. Musculoskeletal pain in the Netherlands: prevalences, consequences and risk groups, the DMC(3)-study. Pain. 2003. 102:167-178
10. Senbursa G. et al. Comparison of conservative treatment with and without manual physical therapy for patients with shoulder impingement syndrome: a prospective, randomized clinical trial. Knee Surg Sports Traumatol Arthro. 2007. 15:915-921
11. Tate A, et al. Comprehensive impairment-based exercise and manual therapy intervention for patients with subacromial impingement syndrome: a case series. JOSPT. 2010. 40:474-491.
12. Winters J. et al. The long-term course of shoulder complaints: a prospective study in general practice. Rheumatology. 1999. 38:160–3
13. Wofford J. et al. Patient characteristics and clinical management of patients with shoulder pain in U.S. primary care settings: secondary data analysis of the National Ambulatory Medical Care Survey. BMC Musculoskelet Disord 2005. 6:4.