

Neck Pain Background Information
Neck pain affects 10-15% of the population at any one time, with a lifetime incidence of 22-70% (1). Only 6% of patients with neck pain report resolution of symptoms at one year (2).
A recent systematic review demonstrated the prognosis from idiopathic neck pain is poor (3) and 50-75% of patients with neck pain will report symptoms at 1 and 5 year follow up (4).
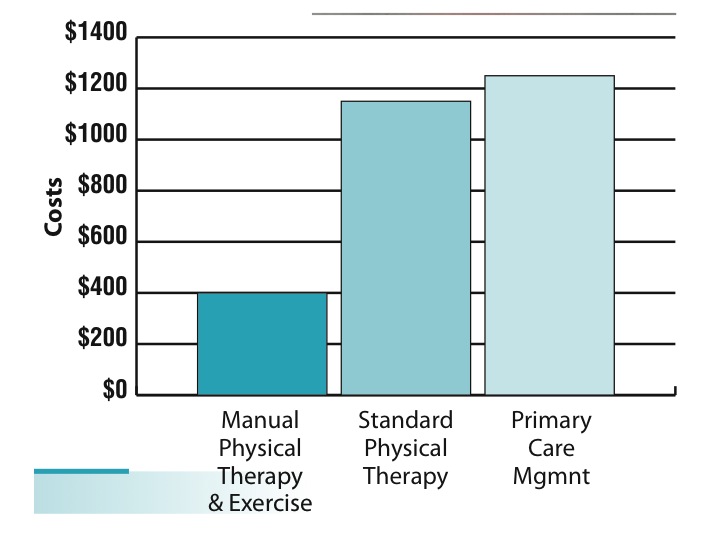
Evidence suggests the utilization of manual therapy and exercise is a more cost effective intervention compared to primary care management alone or standard physical therapy (see graph). (5)
Our effectiveness in treating patients increases as we match interventions to a patient’s signs and symptoms. Evidence suggests outcomes are improved by correctly matching each Physical Therapy intervention to a specific patient category see below.(6)
Patients with mechanical neck pain, cervical radiculopathy, and cervicogenic headaches can benefit from Physical Therapy interventions including manual therapy and exercise to reduce pain and improve disability.
Physical Therapy Interventions for Neck Pain
Exercise and Conditioning

Patients within this category may display lower pain and disability levels and report a longer duration of symptoms.
Exercises will aim to improve muscle function within the deep cervical flexors and scapular muscles.
A recent systematic review provided Level 1 evidence on the benefits of exercise for patients with mechanical neck pain.(7)
Strong evidence supports the utilization of proprioception and strengthening exercises for patients with recurrent or chronic neck pain.(8)
Headaches
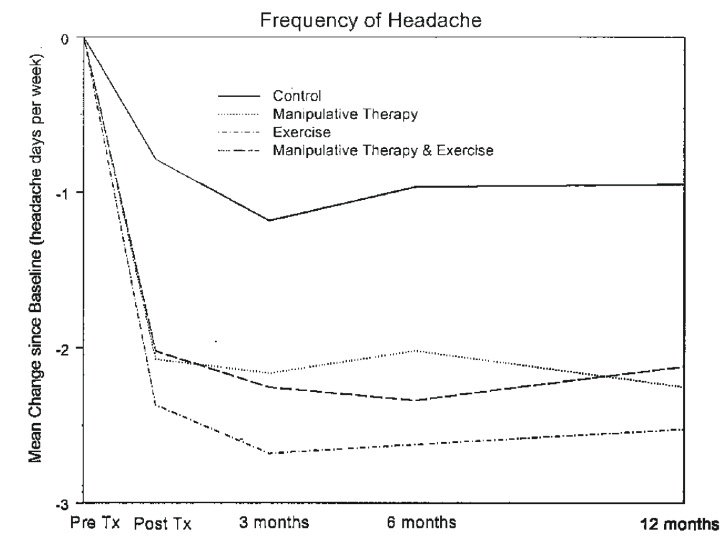
A recent Cochrane review documented the improved effectiveness of manual therapy and exercise over manual therapy alone in patients with neck pain with or without headaches.(10)
Authors report the benefit of cervical manipulation on reducing head- ache intensity and frequency in patients with headache.(9)
The utilization of manual therapy and cervical strengthening has been show to reduce pain, disability, and headaches over both the short and long term (see graph) (11).
Neck and Arm Pain/Cervical Radiculopathy
Centralization
Patients within this category include those who have signs and symptoms of nerve root impingement or radicular symptoms.
Studies demonstrate 26% of patients with cervical radiculopathy who undergo surgery continue to experience high levels of pain at a 1-year follow-up.(12) Studies also suggest that patient outcomes may be superior with conservative management versus surgical interventions.(13, 14)
Physical therapy interventions consisting of manual therapy (17), cervical traction (15, 16), and cervical centralization exercises have been shown to decrease pain and improve function in this population.
Recently authors reported 91% of patients with cervical radiculopathy who underwent treatment of manual physical therapy, cervical traction and strengthening exercises showed significant functional improvement. (17).

Pain Control
This subgroup comprises patients with acute or traumatic onset of neck pain, including whiplash injury, and those presenting with high levels of pain and disability.
Physical therapy interventions for this category aim to decrease pain and allow transition into other subgroups for treatment to reduce disability.
Evidence suggests utilization of thoracic spine manipulation18, cervical spine mobilizations19, neck active ROM exercises20, gentle soft tissue massage(21), and physical modalities such as TENS (22).
Interventions matched to patient’s signs and symptoms within the category demonstrate greater changes in pain and disability than unmatched interventions (6).
Mobility
Patients within this group include those with symptoms proximal to the elbow, an acute onset (<30 days), and are younger than 60 years old.(6)
Evidence supports the utilization of both cervical and thoracic mobilization/manipulation, with exercise, to restore mobility, decrease pain, and improve function. (1, 22, 23)
Utilization of manual therapy can reduce long term management costs by as much as 2/3 in comparison with exercises or medical management alone. (24)
References
Childs, J. Cleland, J. et al. Neck Pain: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health From the Orthopaedic Section of the American Physical Therapy Association. J Orthop Sports Phys Ther 2008;38(9):A1-A34.
Picavet HS, Schouten JS. Musculoskeletal pain in the Netherlands: prevalences, consequences and risk groups, the DMC(3)-study. Pain. 2003;102:167-178.
Hush JM, Lin CC, Michaleff ZA, Verhagen A, Refshauge KM. Prognosis of acute idiopathic neck pain is poor: a systematic review and meta-analysis. Arch Phys Med Rehabil 2011;92:824-9
Carroll L. Hogg-Johnson, S. et al. Course and Prognostic Factors for Neck Pain in the General Population. Spine. 2008;33(4):S75–S82.
Korthals-de Bos IB, Hoving JL, van Tulder MW, et al. Cost effectiveness of physiotherapy, manual therapy, and general practitioner care for neck pain: economic evaluation alongside a randomized controlled trial. BMJ. 2003.
Fritz JM, Brennan GP. Preliminary examination of a proposed treatment-based classification system for patients receiving physical therapy interventions for neck pain. Phys Ther. 2007;87:513–524.
Kay, T. Gross, A. et al. Exercises for mechanical neck disorders. Cochrane Database of Systematic Reviews. 2005. CD004250.
Sarig-Bahat, H. Evidence for exercise therapy in mechanical neck disorders. Manual Therapy. 2003;8:10-20.
Nilsson, N. Christensen, J. et al. The effect of cervical manipulation on cervicogenic headache. J Manip Phys Ther. 1997;20:326-330.
10. Gross, A. Hoving, J. et al. A Cochrane Review of Manipulation and Mobilization for Mechanical Neck Pain. Spine 2004;29:1541–1548
11. Jull, G. Trott, P. et al. A Randomized Controlled Trial of Exercise and Manipulative Therapy for Cervicogenic Headache. Spine. 2002;27(17):1835–1843
12. Heckmann JG, Lang CJ, Zobelein I, Laumer R, Druschky A, Neundorfer B. Herniated cervical intervertebral discs with radiculopa- thy: an outcome study of conservatively or surgically treated patients. J Spinal Disord. 1999;12:396-401.
13. Honet JC, Puri K. Cervical radiculitis: treatment and results in 82 patients. Arch Phys Med Rehabil. 1976;57:12-16.
14. Sampath P, Bendebba M, Davis JD, Ducker T. Outcome in patients with cervical radiculopathy. Prospective, multicenter study with independent clinical review. Spine. 1999;24:591-597.
15. Graham N, Gross AR, Goldsmith C. Mechanical traction for mechanical neck disorders: a systematic review. J Rehabil Med. 2006;38:145-152.
16. Moeti P, Marchetti G. Clinical outcome from mechanical intermittent cervical traction for the treatment of cervical radiculopathy: a case series. J Orthop Sports Phys Ther. 2001;31:207-213.
17. Cleland, J; Whitman, J; Fritz, J; Palmer, J. Manual Physical Therapy, Cervical Traction and Strengthening Exercises in Patients with Cervical Radiculopathy: A Case Series. J Orthop Sports Phys Ther. 2005:35(12):802-809.
18. Gonzalez-Iglesias, J., Fernandez-de-las-Penas, C., Cleland, J., & Gutierrez-Vega, M. (2009). Thoracic spine manipulation for the
management of patients with neck pain: a randomized clinical trial. Journal of Orthopaedic & Sports Physical Therapy, 39(1), 20-27.
19. Conlin A, Bhogal S, Sequeira K, Teasell R. Treatment of whiplash- associated disorders, part I: non-invasive interventions. Pain Res Manag. 2005;10:21-32.
20. Rosenfeld M, Gunnarsson R, Borenstein P. Early intervention in whiplash-associated disorders: a comparison of two treatment protocols. Spine. 2000;25:1782-1787.
21. Skyba D, Radhakrishnan R, Rohlwing J. Joint manipulation reduces hyperalgesia by activation of monoamine receptors but not opioid or GABA receptors in the spinal cord. Pain 2003;106:159e68.
22. Cassidy, J.D., Lopes, A.A., Young-Hing, K. The immediate effect of manipulation vs mobilization on pain and range of motion in the cervical spine: a randomized control trial. Journal of Manipulative and Physiological Therapeutics. 1992. 15:9.
23. Cleland, J.A., Mintken, P.E., Carpenter, K., Fritz, J.M., Glynn, P., Whitman, J., Childs, J. Examination of a clinical prediction rule to identify patients with neck pain likely to benefit from thoracic spine thrust manipulation and a generally cervical range of motion exercise: multi-center randomized control trial. Physical Therapy. 2010. 90: 9.
24. Ingeborg, B.C., Korthals-de Bos, Hoving, J.L., Tulder, M.W., Rutten-van Molken, M., Ader, H.J., CW de Vet, H., Koes, B.W., Vondelling, K., Bouter, L.M. Cost effectiveness of physiotherapy, manual therapy, and general practicioner care for neck pain: economic evaluation alongside a randomized control trial. British Medical Journal. 2003. 326:911