

Low Back Pain Background Information
Low back pain is a common disorder affecting up to 90% of people in the lifetime and is the 2nd most common reason people seek medical attention(1,2).
Our health care system spends an average of over $90 billion dollars on low back pain largely from increases in surgical procedures, injections, and medications(3). Unfortunately, this rise in costs has not been associated with any improvements in low back pain outcomes.
Low back pain is a leading cause of missed work and sick days. Patients missing 6 months or more of work have only a 0-2% chance of returning to work.
It is important to note <5% of low back pain is related to serious pathology with the vast majority (85-95%) being non specific in nature. Given these results conservative care is first line management of low back pain6.
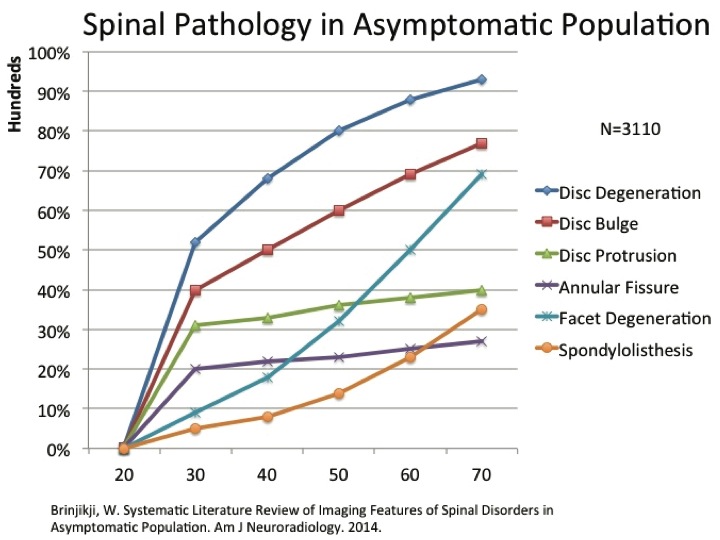
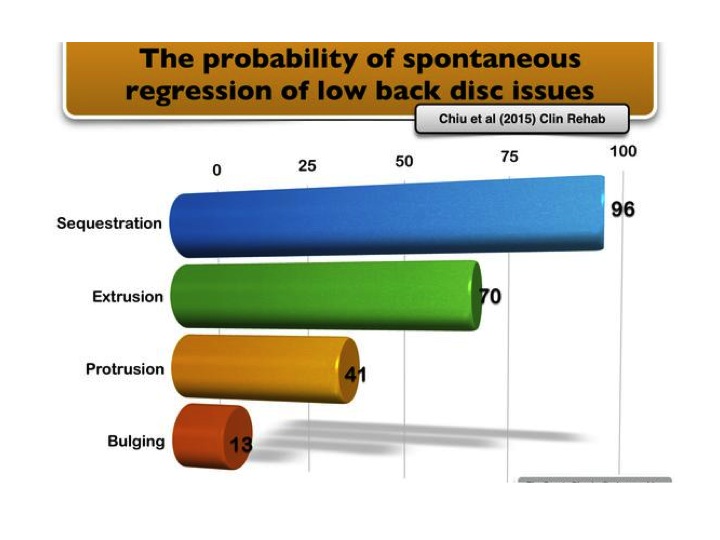
Multiple authors have documented the high rate of false positive MRI results. The incidence of pathology rises steeply in asymptomatic individuals over age 30(8). Interestingly, the most serious lumbar disc injuries also have the greatest probability of healing/regression with conservative management on follow up MRI(9).
Physical Therapy Treatments for Low Back Pain
Many interventions used in Physical Therapy including manual therapy, exercise, and traction previously demonstrated equivocal or limited evidence for LBP. Authors report LBP is a heterogeneous condition and studying a large sample of patients with LBP leads to a wash out effect. Conversely, authors now recommend studying more homogenous groups (subgroups) of patients.
The non specific nature of low back pain limits the effectiveness of Physical Therapy interventions designed to treat an anatomical structure (intervertebral disc or nerve). In addition, many interventions used in Physical Therapy including manual therapy, exercise, and traction previously demonstrated equivocal or limited evidence for LBP. Authors report LBP is a heterogeneous condition and studying a large sample of patients with LBP leads to a wash out effect. Conversely, authors now recommend studying more homogenous groups (subgroups) of patients.
Experts currently recommend treating patients based on their signs and symptoms which has been documented to provide superior outcomes compared to other approaches(5).
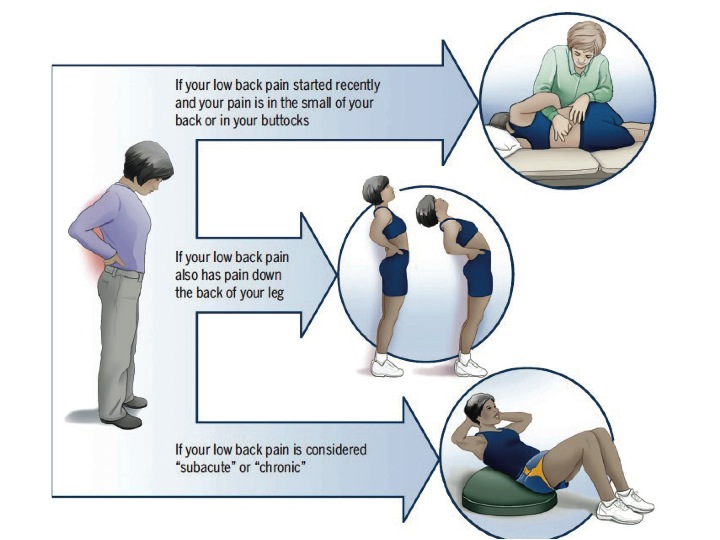
The four sub groups of treatment for acute low back pain include:
Manipulation
Stabilization Exercise
Direction Specific Exercise
Traction
Physical Therapy Evidence for Low Back Pain
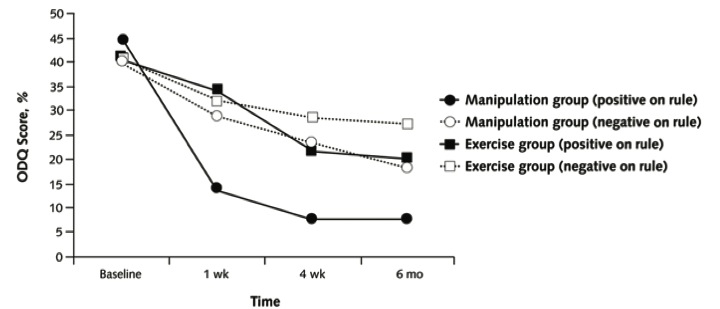
Spinal manipulation followed by stability exercises has been shown to rapidly reduce disability with benefits noted up to 6 months compared to other treatments. The number needed to treat for this intervention is 1-2 indicating for every patient receiving manipulation an additional patient will improve vs. exercise alone(7).
In a randomized controlled trial of spinal stabilization training compared to usual medical management. Hides et al. reported reduced recurrence (30% vs. 84%) and future medical care (42% vs. 15%) in the stabilization group. The risk of recurrence for the medical management group remained high up to 3 years(10). There does not seem to be a greater effect of local versus global stabilization training among patients who meet the spinal stabilization sub group criteria (11).
In a large, randomized controlled trial Long et al. reported the reduction of back and leg pain, disability, medication use, and psychosocial variables including depression when patients with a directional preference for lumbar exercises were matched to their respective directions(12). Browder et al. showed a reduction in pain and disability at both short and long term outcomes when manual therapy was combined with direction specific exercises (extension oriented treatment effect)(13).
Traction is a less commonly indicated for acute low back pain but a sub group of patients who may benefit from this intervention early include patients with signs of nerve root compression, contralateral straight leg raise(14).
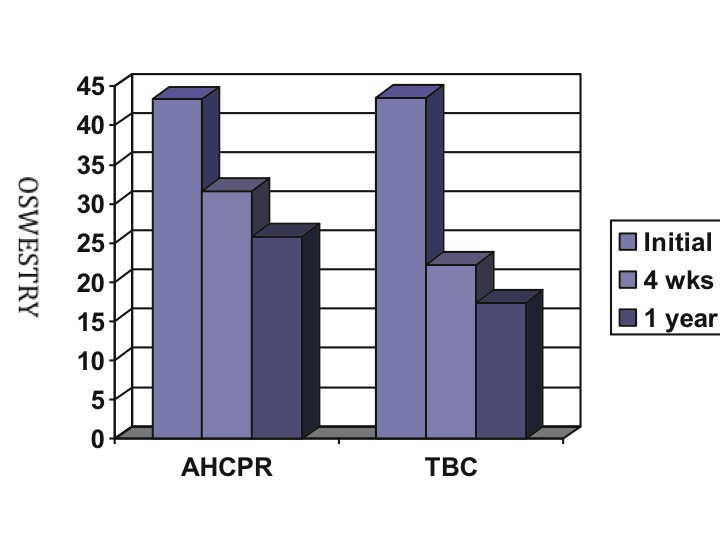
The treatment based classification system (TBC), based on a patient’s signs and symptoms, is less expensive ($774 vs. $1004) and more effective at improving pain, disability, and return to full time work status compared to national medical guidelines (AHCPR)(15).
When To Seek Physical Therapy Care
“Non specific LBP should not be viewed as a homog- enous condition. Outcomes can be improved when sub grouping is used to guide treatment decision-making.”5
Patient’s with acute low back pain without red flags should be referred immediately to Physical Therapy for appropriate sub grouping and management.
References
1. Patel, A. et al. Dianosis and Management of Acute Back Pain. Am Fam Physician. 2000 Mar 15;61(6):1779-1786.
2. Hart, L. et al. Physician office visits for low back pain. Frequency, clinical evaluation, and treatment patterns from a U.S. national survey. Spine. 1995. 20(1):11-9.
3. Luo, X. et al. Estimates and Patterns of Direct Health Care Expenditures Among Individuals With Back Pain in the United States. Spine. 2004. 29(1):79-86.
4. Stewart, W. Lost Productive Time and Cost Due to Common Pain Conditions in the US Workforce. JAMA. 2003. 290(18):2443-2454
5. Brennan, G. et al. Identifying Subgroups of Patients With Acute/Sub acute “Nonspecific” Low Back Pain: Results of a Randomized Clinical Trial. Spine. 2006.
6. Deyo, R. et al. What Can the History and Physical Examination Tell Us About Low Back Pain? JAMA. 1992. 268(6):760-766.
7. Childs, J. Fritz, J. et al. A Clinical Prediction Rule To Identify Patients with Low Back Pain Most Likely To Benefit from Spinal Manipulation: A Validation Study. Annals of Int Med. 2004/920-928.
8. Brinjikji, W. Systematic Literature Review of Imaging Features of Spinal Disorders in Asymptomatic Population. Am J Neuroradiology. 2014.
9. Chiu, C. et al. The probability of spontaneous regression of lumbar herniated discs. A systematic review. Clinical Rehab. 2015, Vol. 29(2) 184–195
10. Hides, J. et al. Long-Term Effects of Specific Stabilizing Exercises for First-Episode Low Back Pain. Spine. 2001. 26(11):243-248.
11. Koumantakis,G.etal.TrunkMuscleStabilizationTrainingPlusGeneralExercise Versus General Exercise Only: Randomized Controlled Trial of Patients With Recurrent Low Back Pain. Phys Ther. 2005;85:209 –225
12. Long, A. Donelson, R. Does it matter which exercise. A randomized control trial of exercise for low back pain. Spine. 2004;29:23:2593-2602.
13. Browder, D. et al. Effectiveness of an Extension-Oriented Treatment Approach in a Subgroup of Subjects With Low Back Pain: A Randomized Clinical Trial. PT. 2007;87:1608–1618
14. Fritz, J. et al. Is There a Subgroup of Patients With Low Back Pain Likely to Benefit From Mechanical Traction? A RCT and Subgrouping Analysis. Spine. 2007. 32(6):E793-E800.
15. Fritz, J. Delitto, A. et al. Comparison of Classification-Based Physical Therapy With Therapy Based on Clinical Practice Guidelines for Patients with Acute Low Back Pain. A Randomized Clinical Trial. Spine. 2003;1363-1372.